The only organisation in the country that addresses the needs of persons with and affected by epilepsy
by Marina Clarke, Director
An overview of the organization
Epilepsy South Africa is the only national organisation in our country addressing the needs of persons with and affected by epilepsy. The organisation was established in 1967 as the South African National Epilepsy League (SANEL) but changed our name to Epilepsy South Africa in 2002.
Epilepsy South Africa is a full Chapter of the International Bureau for Epilepsy (IBE) with strong ties to IBE Africa and the South African Disability Alliance (SADA).



Our organisation comprises a small virtual National Office with six Branches:
- Epilepsy SA Western Cape based in Cape Town
- Epilepsy SA South Cape/Karoo based in Knysna
- Epilepsy SA Eastern Cape based in East London
- Epilepsy SA Gauteng based in Springs and Johannesburg
- Epilepsy SA Free State & North West based in Parys; and
- Epilepsy SA Mpumalanga & Limpopo based in Dullstroom and Elandsdoorn
We follow a human rights approach to our work and subscribe to the United Nations Convention on the Rights of Persons with Disabilities (UN CRPD) which was translated at national level to the White Paper on the Rights of Persons with Disabilities (WPRPD). As such advocacy and the development of self-representation is a key element of our work. Our services are largely psychosocial and include
- Social development (e.g. counselling, residential care, community outreach and support groups);
- Economic development (protective workshops, income generation projects, open labour market employment and entrepreneurial development);
- Skills development (learnership, internships and short courses).
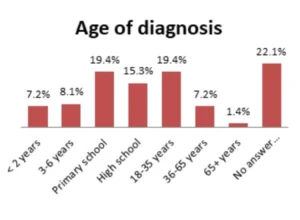
Percentage of the South African population with epilepsy and the age range with the highest incidence
While some data exists about the prevalence of disability, there is a significant lack of data about epilepsy as this information is not captured by Government. As such, we base our assumptions on the statistics provided by the World Health Organisation (WHO) that one in every hundred people in a developing country like South Africa has epilepsy.
Through a survey we conducted in 2020 we established an apparent trend for epilepsy diagnoses in the younger population.
Persons with epilepsy are one of the most stigmatised groups in South Africa with several myths and misconceptions. These include the well-known references to curses and magical spells as causes of epilepsy, but also extend to interesting suggestions for treatment such as pouring water over a person during a seizure or burning selected herbs to cure the person.
As an organisation we believe that awareness and knowledge about the condition are key elements to ensure acceptance and inclusion of persons with epilepsy. While we have several active social media campaigns, we also participate in media interviews and conduct awareness talks and workshops in communities.
Our key calendar event is International Epilepsy Day which is celebrated on the second Monday in February followed in South African by National Epilepsy Week. Other important events include Human Rights Day (24 March), SUDEP Action Day (23 October) and International Day of Persons with Disabilities (3 December).
Our Advocacy Toolkit comprises brochures, posters, video clips and activity material and supports the outreach work of both staff members and self-advocates while our electronic library enables easy access to information about epilepsy.
Access to care and employment for people with epilepsy
Global economic trends have a significant impact on the South African economy as evidenced by less than 2% growth in recent years. The impact is evidenced by increasing unemployment (particularly amongst young people), cutbacks in and redirection of government spending and a significant reduction in funding for social issues. National and international trends impact the opportunities available to persons with and affected by epilepsy and thus access to care and employment.
While Epilepsy South Africa offers limited residential care, we believe in the inclusion of persons with epilepsy in communities, preservation of the family unit and independence. As such, admission to residential facilities is limited to persons requiring a high level of care due to their epilepsy and comorbidities/disabilities, as well as the ability of family members to provide the required levels of care. We thus offer support to families and communities to enable persons with epilepsy to actively participate in their communities. In addition to counselling services we also assist with access to social security and services at local level.
In terms of employment Epilepsy South Africa focuses on placement in the open labour market and protective employment, as well as self-employment and entrepreneurship. However, the stigma surrounding epilepsy can be seen in the unwillingness of many persons with epilepsy to disclose their condition despite employment equity legislation.
However, the high unemployment rate in South Africa (currently estimated at 30%) means that most persons with epilepsy remain unemployed and reliant on limited social security, their families and communities.
The legacy of South Africa’s past continues to plague persons with epilepsy given poor education and skill levels. This means that many people do not have the required skills and experience to effectively engage with market requirements. In response, Epilepsy South Africa established skills development services in partnership with government agencies and the private sector with a view to improving the employability of persons with epilepsy.
Myths about epilepsy
The most common myths and misconceptions about epilepsy include:
- Epilepsy is a sign of spiritual possession, a curse or magical activity. This means that persons with epilepsy may have special powers (e.g. foretelling the future).
- Because epilepsy is contagious contact with anybody who has epilepsy or a family member/friend with epilepsy must be avoided.
- Epilepsy affects intelligence which means that children with epilepsy cannot attend school nor can people with epilepsy learn skills such as driving.
- It is important to put something in the person’s mouth during a seizure to prevent them from swallowing their tongue and dying.
- Seizures are always medical emergencies and you should call an ambulance immediately.
- There is only type of seizure – a convulsion.
- You can stop a seizure by lighting a flame and letting the person inhale the smoke. Other suggestions include pouring a bucket of water over the persons.
- People with epilepsy should be pitied, feared or ignored.
- People with epilepsy are lazy and an employment risk.
Some of the ways epilepsy can be managed
While there is no cure for epilepsy the condition can be effectively treated. The objective of any treatment is to control seizures with the least side effects.
Effective treatment requires a proper diagnosis by a medical practitioner (ideally a neurologist). Diagnosis is based on an accurate medical history (usually provided by both the individual and family members) and one or more tests (e.g. EEG or MRI scans).
The most common treatment for epilepsy is anti-seizure medication. Unfortunately, such medication may have unpleasant side effects and requires adjustment over a period of time to find the most suitable drugs and dosage for the individual. As a result, some people with epilepsy feel that the treatment is not working or unpleasant and opt to stop taking the medication. Any changes in treatment must be discussed with your doctor.
A medical investigation will determine whether persons with epilepsy are suitable candidates for other forms of treatment, e.g. surgery, the ketogenic diet or Vagus Nerve Stimulation (VNS).
While the need for medical treatment is obvious, persons with epilepsy are ultimately responsible for managing their condition. This not only requires adherence to treatment (e.g. taking medication as prescribed), but also through lifestyle management as this supports the medical treatment and contributes to overall wellness.
Lifestyle management includes a healthy diet, regular exercise, good sleeping habits and stress management. It is important that persons with epilepsy identify their individual seizure triggers and take action to avoid or limit exposure to these. Keeping a seizure diary is helpful in identifying triggers which vary greatly from person to person. Triggers may include weather (e.g. high/low temperatures), specific foods (e.g. caffeine or sugar), alcohol and recreational drugs, flickering lights (applicable only to persons with photosensitive epilepsy), smells, hormonal changes (e.g. menstrual cycles and menopause) and many others.
By keeping a seizure diary you will record what happened before, during and after a seizure which will help you to identify potential seizures. Epilepsy South Africa offers a free seizure diary which can be downloaded from the Epilepsy Information section of our website www.epilepsy.org.za.
Can epilepsy be prevented?
It is impossible to determine the cause of epilepsy in approximately three quarters of cases. As such, it is not always possible to prevent epilepsy. However, some key causes of epilepsy include illness (e.g. meningitis or encephalitis), head trauma (especially cerebral haemorrhage), drug and alcohol abuse, tumours, biochemical imbalances and degeneration (i.e. ageing).
Preventative measures include:
- Taking precautions to avoid head trauma (e.g. wearing a seat belt in vehicles and protective equipment when playing sport);
- Regular medical assessments to ensure early detection of high-risk conditions; and
- Responsible behaviour (e.g. limiting alcohol intake).
The redirection of available funding to Covid-19 interventions and delays in processing previously agreed funds reduced the available funding for the work of Epilepsy South Africa. In addition, the economic hardships resulting from strict lockdown protocols resulted in individuals no longer able to support our work financially. Organisational income generation activities (e.g. retail and service provision) were also curtailed. These factors combined to place significant strain on the financial wellbeing of the organisation as a whole.
Our service delivery was negatively impacted by prescribed lockdown protocols which limited interaction between people. As such, our community outreach came to a virtual standstill with support only available telephonically or online. Support groups could obviously not meet and virtual meetings proved challenging given the high cost of data in South Africa and the lack of access to technology.
Persons employed in our protective workshop were not able to work which reduced their income significantly. Emergency relief support proved to be ineffective and inaccessible to many.
However, the pandemic and accompanying lockdown also helped our organisation to find creative new ways such as hosting virtual meetings with a significant reduction in costs.
——————————
The World Health Assembly (WHA) adopted Resolution 68.20 in 2015 creating worldwide focus on epilepsy. This led Epilepsy South Africa to establish a project to ensure implementation through the creation of a National Epilepsy Task Force to develop a National Epilepsy Plan.
The WHA decision to adopt Resolution 73.10 in November 2020 was a landmark event. Calling for the development of global action plans to combat epilepsy and neurological disorders was a first. The Resolution resulted from the sustained efforts by the International League Against Epilepsy (ILAE) and International Bureau for Epilepsy (IBE). Epilepsy South Africa is the South African Chapter of the IBE and thus supported these efforts.